A comparative study of zoledronic acid and once weekly Alendronate in the management of acute Charcot arthropathy of foot in patients with diabetes mellitusCharcot arthropathy (CA) is a chronic and progressive disease of bone and joints, characterized by painless bone and joint destruction in limbs that have lost sensory innervation. The main cause of CA is diabetic polyneuropathy with the joints of foot being most commonly affected. The condition is rare, however, affecting perhaps only 1% of all people whose diabetes is complicated by neuropathy. The actual incidence of CA is perhaps greater than that reported. 1] The diagnosis of CA is delayed or missed in as many as 25% of patients because it is not widely recognized by non-specialists. The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control2] The failure to identify the condition in its early phases is in part responsible for gross deformity that follows continued weight bearing. The pathogenic mechanisms of CA are not clear, one possible mechanism being reduced bone mineral density, probably as the result of increased bone turnover. The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control3,The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control4] Management of CA depends on the clinical stage. Immobilization with the total contact cast (TCC) is considered the gold standard in initial treatment of Acute CA. The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control5,The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control6] Bisphosphonates such as pamidronate and alendronate have shown good efficacy for the treatment of acute CA. The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control7] Patients treated with intravenous pamidronate were found to have significantly reduced skin temperature, reduction in bone-specific alkaline phosphatase and urinary deoxypyridinoline, and reduced bone turnover. The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control8,The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version. Destroy user interface control9] In another randomized controlled trial The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control10] treatment with oral alendronate was associated with a significantly greater reduction in foot temperature. Till the date of this writing, no study was done to assess the efficacy of Zoledronic acid infusion in patients with acute CA of foot. We therefore, did a randomized comparative study to assess and compare the clinical and scintigraphic response in patients with acute CA of foot to two types of bisphosphonate therapy-single dose Zoledronic acid injection and oral weekly Alendronate. Materials and Methods This single center prospective comparative study was done in Podiatry clinic, Department of Endocrinology, Diabetes and Podiatry, Amrita Institute of Medical Sciences, Cochin, Kerala, India between May 2007 and April 2009. Patients attending the Endocrinology and Podiatry clinic with history of diabetes mellitus (under treatment) and/or recent or previous venous plasma glucose values satisfying the American Diabetes Association criteria for diagnosis of diabetes mellitus, aged 20-80 years with Acute CA as suggested by clinical features are taken for study. Written informed consent was obtained from the study participants. The study was approved by the institutional ethics committee. Acute CA is defined by: Presence of hot swollen foot with or without redness of the overlying skin after the exclusion of conditions resembling CA (discussed below). Temperature of the foot was measured using an infrared thermometer at the site of maximum deformity and temperature on the affected foot and at the corresponding point on the contra-lateral foot. An increase of 4°F or more compared to the similar site on the contra-lateral foot was taken as the indicator of active disease. During the follow-up, foot temperatures were measured at 10 minutes, 15 minutes, and 20 minutes after the soft roll crepe bandage or total contact cast were removed and an average of three readings was taken. Patients were asked to rest supine for the period of measurements. Any patient with fever, elevated leucocyte counts, Serum creatinine ≥3 mg/dL (checked on two different occasions), clinical or radiological features suggestive of Osteomyelitis of foot bone, clinical or radiological evidence of peripheral vascular occlusive disease, presence of foot ulcer, hypocalcaemia, any patient with planned dental procedure, patients who were previously treated for CA of foot or who are on Bisphosphonate therapy for any reason, any surgical procedure of the affected foot in the past, patients with Rheumatoid arthritis, gout were excluded from the study. The patients were randomized alternately into two groups. Group Z-patients in this group received Zoledronic acid injection 5 mg. as intravenous infusion (diluted in 100 ml. normal saline infused over 30 minutes) after hospital admission along with total contact casting. If serum creatinine was ≥2 mg/dL then the dose of Zoledronic acid was reduced to 2.5 mg. Group A – patients in this group received Tab. Alendronate 70 mg. once a week till the complete clinical resolution of acute CA along with total contact casting. Patients were asked to remain upright for at least 30 minutes after taking the medication. A total contact cast was applied to all patients for the affected foot, with the help of a trained podiatry assistant. They were instructed to strictly offload the affected limb with the help of a walker. They were trained to walk with the help of walker by the physiotherapist who is trained in the management of patients with diabetic foot problems. All patients were followed up once a month. During each visit the temperature of the normal and the affected feet were measured and compared. The compliance with medication was ensured during each visit in patients belonging to Group A. The glycemic control was assessed using morning fasting plasma glucose and 2-hours postmeal plasma glucose levels. Patients were advised to bring their record of home blood glucose monitoring. Dose adjustments of oral hypoglycemic agents and/or insulin were done based on the home blood glucose values and the hospital venous plasma glucose values. Primary End Point of the study was Complete clinical resolution of acute CA as defined by a temperature difference between normal and affected foot <1°F checked on two different occasions. Partial clinical resolution was defined as temperature difference between normal and affected foot ≥1°F and <2°F checked on two different occasions. Incomplete clinical resolution was defined as temperature difference between normal and affected foot ≥2°F and ≤4°F checked on two different occasions. Patients were followed up till the clinical resolution of acute stage of CA. If the patient had at least 2 follow-up visits per month and withdrew from study before complete clinical resolution of acute CA, then the last visit details were taken into account to define the clinical resolution of acute CA (partial or incomplete resolution). If the patient had <2 follow-up visits, the patient was considered as withdrawn from the study. Ankle brachial index (ABI) was measured in both limbs to access the vascularity. Vibration perception threshold (VPT) was measured using Biothesiometer. A three phase skeletal scintigraphy was done for all patients at the time of diagnosis, after 3 months of starting of treatment and/or at the completion of study. The procedure of scintigraphy was as follows: 15mci of 99mTc MDP (Methylene bisphosphonate) injection was given intravenously. Immediate vascular, soft tissue phase images and delayed skeletal phase images were acquired using high resolution collimators on a dual head variable angle gamma camera. Initial dynamic phase or vascular phase-was acquired at two seconds per frame for one minute. This was followed by immediate planar soft tissue image or soft tissue phase for next two minutes. Three hours later skeletal phase images of foot and ankle were acquired. All the scintigraphy images were analyzed independently by two consultants in the department of Nuclear medicine at our institute, who were blinded regarding the clinical details and the treatment of the patients. Visual scoring of the radioactivity in the three phases was done as: 0-No activity, 1-Mild activity, 2-Moderate activity and 3-Marked activity. The final score was calculated by adding the scores in all the three phases. Hence the minimum score was 0 and the maximum was 9. Quantitative scoring was done as follows: Isotope uptake in a standardized area over the affected foot was quantified for the skeletal phase. This was considered as Target. As controls, isotope uptake was also measured over the identical area of the contra-lateral foot. If the patient had a healed Charcot or peripheral vascular disease on the contra-lateral foot the standardized control area was selected from the unaffected site on the foot. This was considered as non-target. The target to non-target ratio (T:NT) was calculated by dividing the uptake in affected foot by that of contra-lateral foot. T:NT = (CF/CN) Χ 100 CF - Count of detected impulses over the affected foot; and CN - Count of detected impulses over unaffected site in normal foot. These calculations were done for the baseline scintigraphy and for the scintigraphy taken at the end of the study period. Percentage reduction in the scintigraphic score was calculated as follows: 100 - (FT:NT/IT:NT Χ 100) FT:NT - T:NT of scintigraphy at the end of study; IT:NT - T:NT of baseline scintigraphy Figure 1: 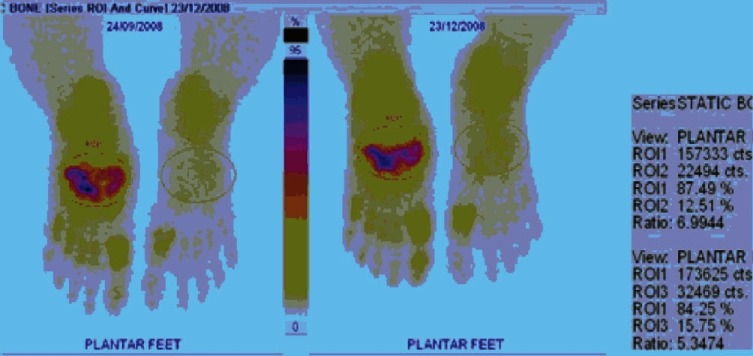 Percentage of reduction in scintigraphic score = 100 - (FT: NT / IT: NT x 100) For this Lesion it is 100 - (6.99 / 5.02 x 100) = 28% The quantative scoring was based on previous studies done in acute CA. The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control12,The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control13] Based on the reduction in the target to non-target ratio from baseline scintigraphy to that at the end of study period, patients were classified as follows: Significant scintigraphic resolution-if there is more than 50% reduction in target to non-target ratio. Moderate scintigraphic resolution-if there is >25 but ≤50% reduction in target to non-target ratio. Minimal scintigraphic resolution-if there is ≤25% reduction in target to non-target ratio. Biochemical parameters Fasting and Postmeal venous plasma glucose levels were estimated by Hexokinase method and were expressed in mg/dL. Glycosylated Hemoglobin (HbA1c) was estimated at baseline and every 3 months by HPLC method and expressed in percentage (%). Patient's glycemic control was classified based on the baseline HbA1c values as: Good glycemic control- ≤7%, Fair glycemic control- >7% and ≤8%, Poor glycemic control- >8% and ≤10%, Very poor glycemic control- ≥10%. Urine albumin/creatinine ratio was estimated in all patients at baseline after excluding any source of infection and controlling hypertension. An elevated value was reconfirmed on a different occasion 2 weeks apart. The cut off values were as follows: <30 mg/gram-Normal, 30-299 mg/gram-Microalbuminuria, ≥300 mg/gram-Macro albuminuria. Serum creatinine was estimated using Jaffe's method at baseline and at the end of study. The normal range was 0.5-1.4 mg/dL. An abnormal value was reconfirmed on another occasion. All patients underwent evaluation for diabetic retinopathy by an ophthalmologist and diabetic retinopathy was classified according to International classification. Statistical analysis Statistical analysis was done using SPSS 11.0 software. The results were expressed in mean ± Standard Deviation (SD). A P value of less than or equal to 0.05 between the groups was considered to be significant. Comparison between two independent variables was done by Mann-Whitney U test and related variables with Wilcoxon signed ranks test. Comparison between more than two unrelated samples was done using Kruskal Wallis test. Correlation coefficients were calculated using Spearman's correlation. Results In the present study, a total of 45 diabetic patients with acute CA were randomized to receive either of the two forms of treatment-Single dose of intravenous Zoledronic acid injection and total contact casting (Group Z) or Oral Alendronate tablets once a week and total contact casting (Group A) till the resolution of the acute phase, which was assessed clinically. All the patients were clinically diagnosed to have type 2 diabetes mellitus. The median age at the time of diagnosis of CA was 56 years (Range 38-71 years). Around 80% of patients were ≥50 years of age at the time of diagnosis. The median diabetes duration at the time of diagnosis of CA was 15 years. The median duration of diabetic peripheral neuropathy symptoms was 36 months, ranging from 1 year to 6 years. At the time of diagnosis, all the patients had classic signs of acute CA. Table 1 Baseline clinical characteristics of study patients 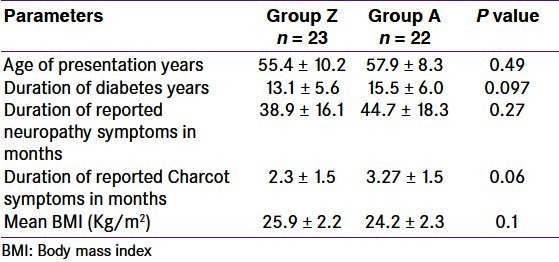 The type of CA was classified according to Frykberg classification. The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control15] Type III CA (53.35%) was the most common type in our study followed by Type IV (28.85%) and Type II (11.05%). There was no patient with Type I CA. Midfoot was most commonly involved (64.4%) in our study than forefoot and hind foot. Right foot was more commonly involved (55.65%) when compared to left foot (44.35%). Thirty three of 45 patients (73.3%) had systemic hypertension, 18 (40%) patients had dyslipidemia (elevated Triglyceride, low HDL according to NCEP ATP-III Guidelines) and 8 patients (17.85%) had previous history of major coronary event (hospitalization for unstable angina or acute myocardial infarction). Two patients (4.4%) had undergone Coronary Artery Bypass Grafting (CABG) and 3 patients (13.6%) had Percutaneous Trans luminal Coronary Angioplasty (PTCA). The median Body Mass Index of the study patients was 25.52 Kg/m2 (Range 19.6-28.7). As per the Asian cut off, The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control16] 11 patients (24.44%) were having normal BMI, 11 patients (24.44%) were overweight and 23 patients (51.11%) were obese. 9 patients (20%) had diabetic cheiro-arthropathy on examination. Sixteen patients (35.6%) had moderate non-proliferative diabetic retinopathy, 4 patients (8.9%) had severe non-proliferative retinopathy and 5 (11.2%) had proliferative retinopathy. Among the baseline investigations, mean Glycosylated Hemoglobin was 8.95 ± 1.69% (range 6.5-13.6%). Sixteen patients (35.6%) had poor glycemic control (HbA1c >8% and ≤10%) and 10 patients (22.2%) had HbA1c >10% [Table 2]. Overall, nearly two-third of the patients had uncontrolled blood glucose levels at the beginning of study and this could have adversely influenced the treatment outcome. Consequently, many of our patients required subcutaneous Insulin injections along with metformin for achieving glycemic control. Among the study patients, 31.15% had normal urine albumin/creatinine ratio and normal creatinine. About 40% patients had micro albuminuria, 17.7% had macro albuminuria and 11.15% had elevated creatinine levels >1.4 mg% and <3 mg% as a creatinine level of ≥3 mg% was an exclusion criteria in the study. Baseline clinical and laboratory parameters did not show any statistically significant difference among the two groups. Table 2 Baseline investigations in study patients 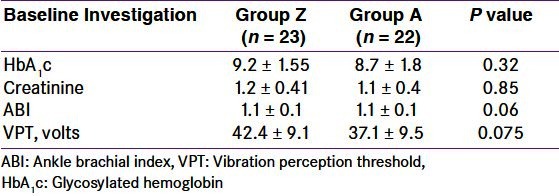 The primary end point of our study was complete clinical resolution of the acute phase of CA as assessed by the temperature difference between the involved foot and the corresponding site on the contra-lateral foot of <1°F. Among the 40 patients (excluding the five patients who withdrew from the study), 30 (75%) had complete clinical resolution. 16 patients in Group Z (76.2%) and 14 patients in Group A (73.7%) had complete clinical resolution (P = 0.85). These patients were included for the final statistical analysis. 5 patients in Group Z (23.8%) and 5 patients in Group A (26.3%) had partial clinical resolution. Time taken for complete clinical resolution The mean number of days taken for complete clinical resolution since the initiation of treatment (either Zoledronic acid or Alendronate) was approximately 122 days. There was no significant difference in number of days required for complete clinical resolution, between the two forms of therapy for acute CA compared in our study [Table 3]. When the cost factor was considered, Zoledronic acid injection was available for Rs.2800 (INR) in our institution. The cost of Alendronate tablet was Rs. 27.31 (INR) for 70 mg dose. When calculated for 26 weeks (182 days-Maximum duration of treatment in Group A) the total cost for Alendronate was Rs. 710. In addition, Zoledronic acid administration required hospital stay for the period of infusion. Table 3 Mean time taken for complete clinical resolution of acute stage of Charcot arthropathy  The time taken for complete clinical resolution of acute CA did not significantly differ among the different types of CA (P = 0.93) or among male and female patients (P = 0.69) and was not correlated to any of the following variables in univariate analysis: Age, duration of diabetes, duration of peripheral neuropathy, duration of Charcot symptoms, vibration perception threshold, BMI or baseline HbA1c. There was a significant reduction in glycosylated hemoglobin levels in both the groups during the study period (P = 0.014 for Group Z and 0.04 in Group A) [Table 4]. Table 4 Comparison of different laboratory parameters at the end of study period among the patients with complete clinical resolution  As expected, all the patients had intense tracer uptake in the skeletal phase of scintigraphy. When the visual scoring was calculated for patients with complete clinical resolution, the baseline scintigraphy score was 6.80 ± 2.33 for Group Z and 5.50 ± 3.39 for Group A (in the visual scale of 0-9). At the end of treatment, the mean score was 3.33 ± 1.98 for Group Z and 2.00 ± 0.1 for Group A [Table 5]. There was more than 50% reduction in the visual score between the baseline and the final scan. The target to non-target ratio in the skeletal phase also showed an average of 40% reduction from the baseline to the final skeletal scintigraphy. When baseline scintigraphy visual score and target to non-target ratio were compared with their final data, respectively, there was a significant reduction seen in both groups. Table 5 Skeletal scintigraphy data of study patients with complete clinical resolution (n = 30)  Table 6 Comparison of skeletal scintigraphy data among the groups  More than 75% of patients in each group who had complete clinical resolution of acute CA also had moderate to significant scintigraphic resolution [Table 7]. However, there was no significant correlation between the baseline scintigraphy score and target to non-target ratio to the duration of treatment. There was no significant correlation between the duration of Charcot symptoms and the baseline scintigraphy score or target to non-target ratio. Probably a serial skeletal scintigraphy might be helpful in understanding the pattern of radiological improvement. Table 7 Scintigraphic resolution in patients with complete clinical resolution 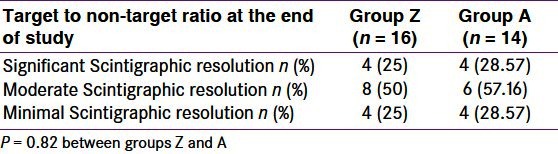 Nine patients in group Z (39.13%) experienced drug induced flu like symptoms which lasted for 24-48 hours after Zoledronic acid injection and subsided with antipyretics. Discussion This is the first single center prospective randomized comparative study to assess the efficacy of two bisphosphonates in diabetic patients with acute CA of foot with respect to complete clinical resolution of the acute stage. The data on the clinical spectrum of CA and the usefulness of bisphosphonate therapy are very limited, given the rarity of the disease. The previous studies on CA were placebo controlled studies using either Pamidronate The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control17,The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version. Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control18] or Alendronate. The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control19] The study by Anderson et al. The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control18] was a retrospective study in which the limb temperature of patients who received Pamidronate therapy was compared with those of control patients. There was a statistically significant reduction in limb temperature in Pamidronate treated patients than in control patients at the end of 48 hours and 2 weeks. Another study using Pamidronate The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control17] was a multicentre double-blind placebo controlled trial, 39 type 2 diabetic patients with active CA received a single infusion of either 90 mg pamidronate or normal saline (placebo) at baseline in addition to standard care of foot immobilization (with scotch cast boot, pneumatic walker, or total contact cast) and bed rest. Foot temperatures fell significantly in both groups at 2 weeks, with a further fall at 4 weeks in the treatment group only, which did not reach statistical significance in comparison with the placebo group. In the randomized blinded study using Alendronate, The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control10] though there was a significant reduction in foot temperature in both the groups (11 Alendronate and 9 control patients), there was no statistically significant difference in between Alendronate and control group. Thus the study design and the results of the previous studies are variable. Nevertheless, the improvement of foot temperature and the decline in bone turnover markers with the use of bisphosphonates favor their use to accelerate the resolution of acute stage. Consequently, the period of immobilization will be reduced which has a direct bearing over the quality of life and glycemic control of an individual with diabetes. Bisphosphonates are pyrophosphate analogs with high affinity for hydroxyapatite and bind directly to mineralize bone. The bound bisphosphonate blocks the surface of bone and prevents osteoclasts from binding to the resorption surface. The bisphosphonates also inhibit osteoclastic activity, reduce the lifespan of the osteoclasts and alter the bone or bone mineral to reduce the rate of dissolution. The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control19] Osteoclast apoptosis was associated with activation of caspase-3–like proteases, loss of mitochondrial membrane potential and classic morphologic changes. Of the bisphosphonates studied (risedronate, pamidronate, clodronate, etidronate, tiludronate, alendronate, and zoledronic acid), zoledronic acid was the most potent inhibitor of farnesyl pyrophosphate (FPP) synthase and caused the greatest increase in caspase-3–like activity at 48 hours after treatment. The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control20] Annual dose of zoledronic acid has been recently proven as an effective approach for the management of osteoporosis. This intravenous dose has several advantages over other bisphosphonates, compliance being the most important. The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control21] We did the present study because of (a) non availability of pamidronate injection in many parts of our country compared to easy access to zoledronic acid (b) faster onset of action of osteoclastic apoptosis by zoledronic acid (which may help in early resolution of acute phase) and (c) improved patient compliance with single dose of zoledronic acid injection. According to Stuck et al. The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control22] age between 55 and 64 years, diabetes duration 6 years or more, hemoglobin-A 1 c 7% or more, renal failure were associated with an increased incidence of CA. Compared with patients without obesity and neuropathy, those with obesity alone were approximately 59% more likely to have incident CA (Odds ratio = 1.589). It was also showed that an elevated HbA1c is associated with a more than 30% increase in risk for CA and renal failure nearly doubled the risk of CA. Our study patients had all the risk factors for the development of CA as concluded in the previous studies. There was no significant difference in number of days required for complete clinical resolution, between the two forms of therapy for acute CA compared in our study. In the study by Armstrong et al. The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control5] the range of cast duration was between 1 month and 1 year. In this longitudinal study, 55 patients were treated with serial total contact casting until the quiescence of acute stage. The mean duration of casting was 18.5 ± 10.6 weeks. The authors concluded that clinical judgment and thermometric data should indicate the appropriate duration of casting regimen. In the study by Sinacore, The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control23] it was shown that all of the acute Charcot fractures, subluxations, or dislocations healed in an average of 86 ± 45 days. Acute Charcot arthropathies of the ankle, hind foot, or midfoot took longer to heal by total contact cast than arthropathies localized to the forefoot. In both the studies, bisphosphonate therapy was not used. Given the heterogeneity of the studies done in CA patients, an ideal study design for assessing the efficacy of different types of bisphosphonate therapy would have been a randomized placebo controlled trial. Also, such a trial should be adequately powered to assess the mean time taken for the clinical resolution of acute stage. Ours can be considered as a pilot study towards this endeavor. Technetium-99 methylene bisphosphonate (99mTc MDP) bone scans are often used in diabetic foot to determine the presence of osteomyelitis. Although highly sensitive, this modality lacks specificity in acute CA foot. Osteomyelitis, fractures and arthritis will all demonstrate increased radiotracer uptake. However, a negative bone scan is strong evidence against the presence of infection. In the present study, three phase 99mTc MDP scan was not utilized for the diagnosis of acute CA. Also, we excluded all the patients in whom there was a clinical or radiological evidence of osteomyelitis. Any patient with a past or recent history of surgery in the affected foot and any patient with clinical or laboratory features suggestive of systemic arthritis or gout were also excluded. Hence, our study patients were selected after careful exclusion of all other possibility for an abnormal radioactivity in the affected foot. In our study, we utilized the three phase 99mTc MDP scan to assess the baseline radioactive uptake in foot bones and to follow-up the patients. Our objective was to see if the three phase 99mTc MDP scan could be used as a surrogate marker to predict the resolution of acute CA. Hence, we devised the visual scoring system involving all the three phases of the skeletal scintigraphy. We also analyzed the bone scan images by calculating the target to non-target ratio which was previously used in a study by McGill et al. The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control12] Since the radioactive uptake reflects the active bone turnover which is expected to continue even after the acute phase is resolved, it is not surprising that a significant uptake was persistent even at the end of complete clinical resolution of the acute phase. In the study by McGill et al., The following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface controlThe following popper user interface control may not be accessible. Tab to the next button to revert the control to an accessible version.Destroy user interface control12] 30% more isotope uptake was present in the affected foot even after 12 months of treatment. Our observation is consistent with that of the above mentioned study. However, the T:NT and the percentage reduction in scintigraphic score should be validated in a larger group of charcot patients. Also, comparison of scintigraphic resolution of acute phase with the reduction in markers of bone turnover like bone specific alkaline phosphatase, serum collagen COOH-terminal telopeptide of type 1 collagen (1CTP), and hydroxyproline will add strength to the current clinical criteria for resolution of acute phase of the disease. In conclusion, our study shows that, both Intravenous zoledronic acid and oral Alendronate had comparable efficacy with respect to the time taken for attaining complete clinical resolution of acute CA of foot. Larger studies and long term follow-up is required to understand the natural history of CA in the phase of emerging newer and effective medical and surgical treatment modalities. Source National Library of Medicine |